MASCC Risk Index Calculator: The Definitive Guide to Febrile Neutropenia Risk Stratification
Febrile neutropenia (FN) remains one of the most frequent and potentially life-threatening complications of myelosuppressive chemotherapy. The MASCC Risk Index is the global standard for triaging these patients safely.

Quick Navigation
- 1. Understanding the MASCC Risk Index
- 1.1 Score Interpretation and Triage
- 2. Clinical Significance of Stratification
- 2.1 Challenges in Manual Scoring
- 3. Evidence-Based Guidelines
- 3.1 International Guideline Endorsements
- 3.2 Statistical Methodology and Logic
- 3.3 Global Validation: Western & Asian
- 3.4 Limitations and Considerations
- 3.5 Future of Stratification: MASCC-LC
- 4. Using the OncoToolkit Calculator
- 5. Impact on Oncology Care
- 6. Frequently Asked Questions (FAQ)
- 7. Accessing the MASCC Calculator
Febrile neutropenia (FN) remains one of the most frequent and potentially life-threatening complications of myelosuppressive chemotherapy, affecting up to 80% of patients with hematologic malignancies and 10–50% of those with solid tumors. The clinical challenge is immediate: when a cancer patient spikes a fever during a neutropenic nadir, the treating team must rapidly decide between safe outpatient management with oral antibiotics and mandatory hospitalization for intravenous therapy. Getting this decision wrong in either direction carries real consequences—unnecessary admissions drive up cost and nosocomial risk, while premature discharge can be fatal.1
The MASCC Risk Index (Multinational Association for Supportive Care in Cancer) is the most widely endorsed scoring system for making this triage decision. Developed through an international collaboration of over 1,200 febrile neutropenia episodes across 15 countries, the MASCC score translates complex bedside assessments into a single number that predicts the likelihood of serious medical complications. At OncoToolkit, we have built a free, mobile-responsive MASCC Risk Index calculator that lets clinicians compute and interpret this score in seconds—right at the bedside, during MDT rounds, or in the emergency department. [2], [3]
1. Understanding the MASCC Risk Index for Febrile Neutropenia
The MASCC Risk Index is a validated clinical scoring system designed to identify adult cancer patients with chemotherapy-induced febrile neutropenia who are at low risk of serious medical complications. It was first published in 2000 by Klastersky, Paesmans, Rubenstein and colleagues in the Journal of Clinical Oncology, derived from a prospective multinational cohort and subsequently validated in an independent dataset. [2], [1]
The score is composed of seven weighted clinical variables assessed at the onset of fever:
| Variable | Criteria | Points |
|---|---|---|
| Burden of febrile neutropenia | No or mild symptoms | +5 |
| Burden of febrile neutropenia | Moderate symptoms | +3 |
| No hypotension | Systolic BP ≥ 90 mmHg | +5 |
| No COPD | Absence of active COPD | +4 |
| Tumor type | Solid tumor or hematologic malignancy without prior fungal infection | +4 |
| No dehydration | No IV fluid requirement | +3 |
| Outpatient status | Outpatient at fever onset | +3 |
| Age | < 60 years | +2 |
The maximum possible score is 26. Note that the "burden of illness" categories (mild = 5 points and moderate = 3 points) are mutually exclusive and not cumulative—clinicians must select one or the other. [4], [2]
1.1 Score Interpretation and Triage Thresholds
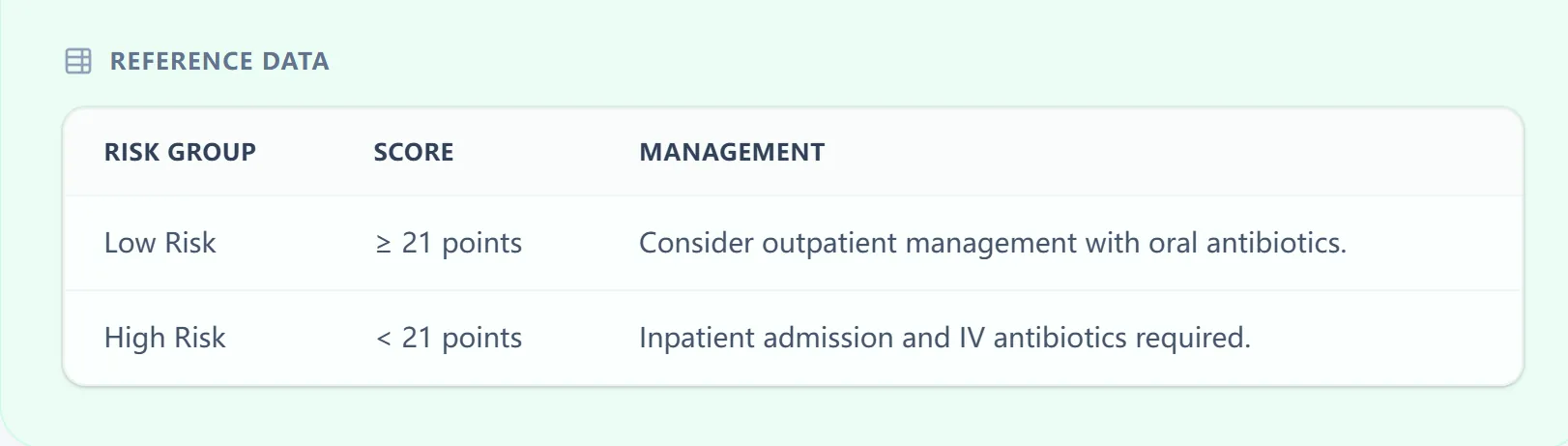
Figure 1. The built-in reference table within our calculator clearly maps MASCC score thresholds to risk categories and management pathways, allowing clinicians to interpret results at a glance.
2. Clinical Significance of MASCC Risk Stratification
Febrile neutropenia management is a time-critical clinical decision. Guidelines from ASCO, IDSA, ESMO, and NCCN all emphasize the need for validated risk stratification at the point of first contact. Without a structured tool, clinicians often default to universal hospitalization—a practice that is both costly and unnecessary for a significant proportion of patients. In a Korean tertiary cancer center study, 38.6% of hospitalized FN patients were retrospectively classified as low risk by MASCC criteria, and over 90% of this low-risk group had outcomes feasible for outpatient management. [5], [3], [6], [7]
2.1 Challenges in Manual Scoring and Bedside Triage
In busy oncology wards and emergency departments, "calculator fatigue" is real. Clinicians must mentally tally seven weighted variables—some of which (like "burden of illness") require subjective judgment—while simultaneously triaging an acutely unwell patient. Paper-based or memory-based scoring is prone to errors in weighting and interpretation, particularly for less experienced physicians or advanced practice providers who may not recall the exact point values. [7]
At OncoToolkit, our MASCC febrile neutropenia calculator is optimized for exactly these high-pressure moments. It is mobile-responsive, requires no login, and produces a scored result with full calculation logic transparency in under 30 seconds. Whether you are prepping for an MDT meeting, running a busy ED shift, or teaching trainees during ward rounds, the tool reduces cognitive load and standardizes the risk stratification process.
3. Evidence-Based Guidelines for the MASCC Risk Index
3.1 International Oncology Guideline Endorsements (ASCO, ESMO, NCCN)
The MASCC Risk Index is one of the most guideline-endorsed risk stratification tools in oncology supportive care:
- ASCO/IDSA (2018 Update): The joint clinical practice guideline for outpatient management of fever and neutropenia explicitly recommends the MASCC score (alongside clinical judgment) for identifying low-risk patients suitable for outpatient therapy. [6], [7]
- IDSA (2010): The Infectious Diseases Society of America's clinical practice guideline for antimicrobial agents in neutropenic cancer patients incorporates MASCC-based risk stratification as a core component of the initial assessment algorithm. [8]
- ESMO: The European Society for Medical Oncology's febrile neutropenia management guidelines reference the MASCC index as the standard tool for risk classification. [3]
- NCCN: The National Comprehensive Cancer Network's Myeloid Growth Factors guidelines endorse validated risk stratification with tools including the MASCC score. [9]
3.2 Statistical Methodology and Weighted Scoring Logic
The MASCC Risk Index uses a weighted point-based scoring system derived from multiple logistic regression analysis. Each of the seven clinical variables was assigned a weight proportional to its independent contribution to predicting low-risk status. The model does not require complex computation—it is a simple summation of points (maximum 26), with the binary cutoff at ≥ 21 distinguishing low-risk from high-risk episodes. [2]

Figure 2. The OncoToolkit calculator displays full clinical context, the primary citation (Klastersky et al., J Clin Oncol 2000), and the formula logic directly alongside the scoring interface.
3.3 Global Validation: Performance in Western and Asian Cohorts
3.3.1 Clinical Outcomes in Western Patient Populations
The original MASCC derivation achieved a positive predictive value (PPV) of 91% for identifying low-risk patients. Subsequent Western validation studies have broadly confirmed these findings. In a pooled analysis across the USA, UK, and South Korea, the MASCC score demonstrated an AUC of 0.772. A 2025 two-center Turkish ED study of 528 FN patients found an AUC of 0.838. [2], [12], [1]
3.3.2 Accuracy and Reliability in Asian Clinical Settings
Importantly, the MASCC score has been validated across multiple Asian populations:
Hui et al. demonstrated superior performance compared to the Talcott model. [14]
Hwang et al. found 90.9% of low-risk patients had outcomes feasible for outpatient care. [7]
Taj et al. achieved a PPV of 93% in a Karachi-based hematology cohort. [9]
3.4 Limitations and Clinical Considerations
No scoring system is perfect, and clinicians should weigh these known limitations:
- Subjective "burden of illness" criterion: Scoring of symptom severity is inherently subjective and may vary between physicians.
- Sensitivity concerns: Serious complications still occur in 15–42% of MASCC-defined low-risk patients in some high-risk subgroups.
- No laboratory parameters: The score relies entirely on clinical variables and does not incorporate biomarkers.
- Adult-derived only: Not recommended for pediatric use. Age criterion is non-discriminatory in children. [20]
3.5 The Future of Risk Stratification: Biomarkers and MASCC-LC
Researchers have explored augmenting the MASCC score with objective biomarkers. The MASCC-LC Model (2025) proposed by Kanter et al. incorporates lactate and CRP, achieving an AUC of 0.995 for 30-day mortality prediction in 269 FN patients. [11]
4. Using the OncoToolkit MASCC Risk Index Calculator
4.1 Inputting Clinical Variables
The calculator presents each MASCC variable as a clearly labeled question with toggle-style buttons. For each criterion, the point value is displayed directly on the button (e.g., "No COPD (+4)"), eliminating any need to memorize weights.
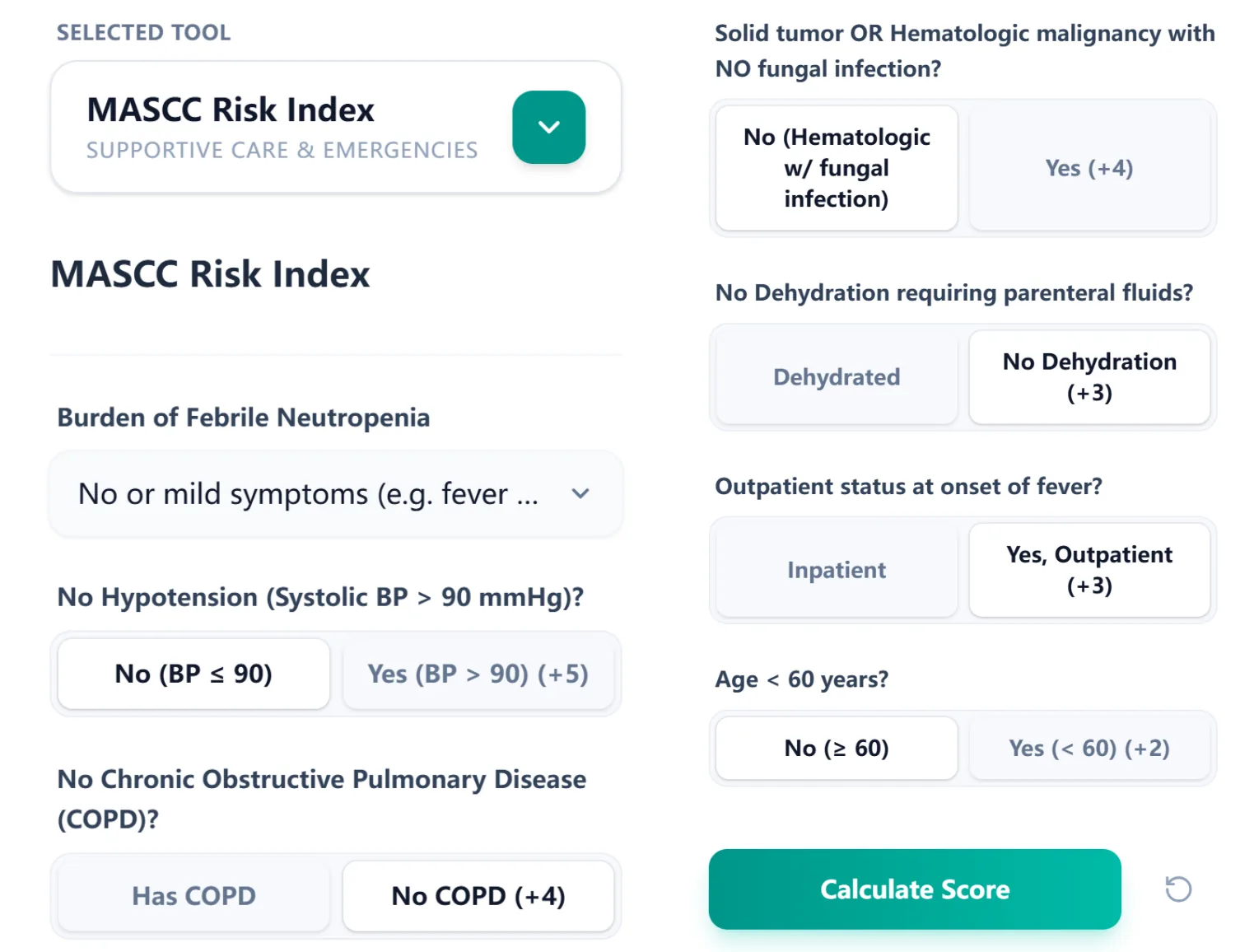
Figure 3. The input interface groups all seven MASCC variables on a single scrollable screen.
4.2 Interpreting Real-Time Results and Logic
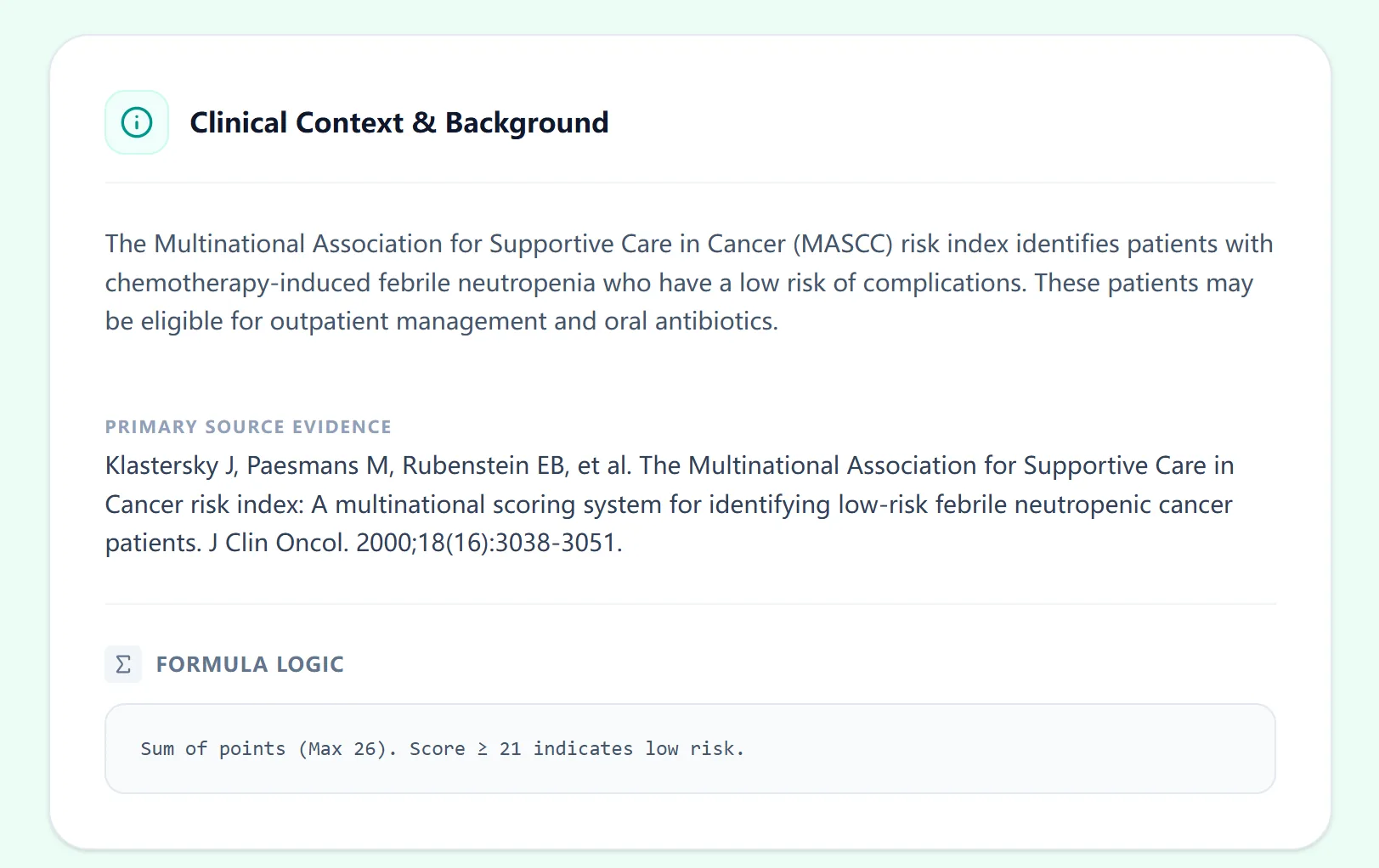
Figure 4. A worked example: this patient scores 15 (High Risk). The logic panel traces exactly which variables contributed.
5. Impact on Oncology Care, Medical Education, and Research
The primary use case is rapid risk stratification at the bedside or in the emergency department. When a patient presents with febrile neutropenia, the calculator can be opened on any smartphone or tablet, completed in under 30 seconds, and used to inform the immediate management decision. [7]
For multidisciplinary team (MDT) meetings, the calculator provides a standardized, reproducible framework for presenting FN cases. Trainees can use it to work through clinical scenarios and develop intuition for the variables that drive risk classification. The expandable calculation logic panel turns every scored case into a teaching moment.
6. Frequently Asked Questions (FAQ)
Can the MASCC Risk Index be used in pediatric patients?
The MASCC score was derived and validated exclusively in adult populations and is not recommended for pediatric use. Pediatric oncology teams should use age-appropriate tools such as the Rackoff rule. [20]
7. Accessing the MASCC Risk Index Calculator
Febrile neutropenia remains an oncologic emergency where speed and accuracy matter. The MASCC Risk Index gives clinicians a guideline-endorsed, globally validated framework to make the admit-or-discharge decision with confidence.
Ready to Stratify Febrile Neutropenia Risk?
Access our guideline-endorsed MASCC calculator for immediate bedside decision support.
Use the MASCC Risk Index Calculator
Free to use. No registration required.
References
- Febrile neutropenia is a life-threatening complication of chemotherapy... Source
- MASCC Risk Index - Neutropenic precautions and risk assessment... Source
- Guidelines in the Management of Febrile Neutropenia for Clinical Practice. Source
- ASCO GUIDELINES Bundle - Outpatient Management of Fever and Neutropenia... Source
- Global guidelines for febrile neutropenia management. Source
- Outpatient Febrile Neutropenia Management - U.S. Pharmacist. Source
- Hwang S, et al. Usefulness analysis of the 2018 ASCO/IDSA guideline... Source
- Fever and Neutropenia in Adults with Cancer - ASCO/IDSA Clinical Practice Guideline Update. Source
- Taj M, et al. Validation of MASCC Score for Risk Stratification... Source
- Sandherr M, et al. 2024 update of the AGIHO guideline on diagnosis and treatment... Source
- Kanter, et al. Improving Prognostic Accuracy of MASCC Score with Lactate and CRP. Source
- Comparison of the MASCC and CISNE scores for identifying low-risk... Source
- Accuracy of MASCC and CISNE scores: A systematic review and meta-analysis. Source
- Hui EP, et al. Evaluation of risk assessment tools in Chinese population. Source
- Prediction of outcome in cancer patients with febrile neutropenia (Hui et al.). Source
- Evaluation of Clinical Profile and Application of MASCC Scoring in India. Source
- Comparison of CISNE and MASCC Score in Predicting Complications in Indonesia. Source
- New scoring system combining WHO ordinal scale and MASCC score - PMC. Source
- Comparison of CISNE and MASCC Score in Predicting Complications (Academia). Source
- Phillips B, et al. Systematic review of discriminatory tools in pediatric FN. Source