PLCOm2012 Lung Cancer Risk Calculator: Identify High-Risk Patients Fast
Calculate individualized 6-year lung cancer risk in seconds. PLCOm2012 calculator for LDCT screening eligibility. Evidence-based, guideline-aligned decision support.
Quick Navigation
- 1. Introduction: Precision in Lung Cancer Screening
- 2. What Is the PLCOm2012 Lung Cancer Risk Model?
- 3. Clinical Significance: Moving Beyond Standard Criteria
- 3.1 Reducing Disparities in Screening Eligibility
- 3.2 Optimizing Clinical Workflow and Cognitive Load
- 4. Evidence and Validation of the PLCOm2012 Model
- 4.1 The Mathematical Foundation
- 4.2 Comparing PLCOm2012 to Bach and Spitz Models
- 5. Clinical Limitations and Implementation Caveats
- 6. How to Use the OncoToolkit PLCOm2012 Calculator
- 7. Guideline-Based Risk Stratification Framework
- 8. Supporting Clinical Care, Education, and Research
- 9. Frequently Asked Questions (FAQ)
- 10. Conclusion: Integrating Risk-Based Screening
Start Here
Open the PLCOm2012 Screening Calculator
Estimate 6-year lung cancer risk, compare with USPSTF-style criteria, and document the LDCT screening discussion.
Next Workflow
PLCO vs Brock vs Lung-RADS
Use PLCO before screening, Lung-RADS for LDCT reports, and Brock/Mayo/Herder after a pulmonary nodule is found.
1. Introduction: Precision in Lung Cancer Screening
Every day, pulmonologists and primary care clinicians face a critical yet frustrating decision: Who should be screened for lung cancer with low-dose CT? The answer seems straightforward—patients at high enough risk to justify surveillance. But in practice, determining that risk requires juggling multiple clinical variables, mental math, and often a vague sense of uncertainty about whether you're applying the right criteria.
For years, screening decisions relied on crude age and pack-year thresholds (the old USPSTF criteria: ages 55–80, ≥30 pack-years). These rules were fast but left many high-risk patients unscreened while subjecting others to unnecessary imaging. The PLCOm2012 Lung Cancer Risk model changes that calculus. At OncoToolkit, we've built a PLCOm2012 Lung Cancer Risk calculator that transforms a complex, multivariable risk assessment into a rapid, transparent decision point—one that aligns with current guideline practice and reduces cognitive load in the clinical workflow.
This article explores what PLCOm2012 is, why it matters for modern lung cancer care, how it compares to alternative risk models, and how our platform enables clinicians to integrate this evidence-based tool seamlessly into screening workflows, education, and quality improvement initiatives.
2. What Is the PLCOm2012 Lung Cancer Risk Model?
The PLCOm2012 model is a validated logistic regression model that quantifies a patient's individualized 6-year risk of developing lung cancer. It emerged from the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial, a large prospective cohort that followed over 150,000 participants and captured detailed demographic, medical, and behavioral data.1
- Age (years)
- Race/ethnicity (accounting for epidemiological variation)
- Education level (socioeconomic proxy)
- Body Mass Index (BMI) (kg/m²)
- COPD history
- Personal history of cancer
- Family history of lung cancer
- Smoking status (current, former, or never)
- Smoking intensity and duration
The model uses coefficients derived from logistic regression to weight each factor and generate a predicted probability. This approach is more granular than fixed cutoffs—it recognizes that a 55-year-old former smoker with a 40-pack-year history and a family history of lung cancer faces substantially different risk than a 60-year-old with a 25-pack-year history and no family history, even if their basic demographics seem similar.
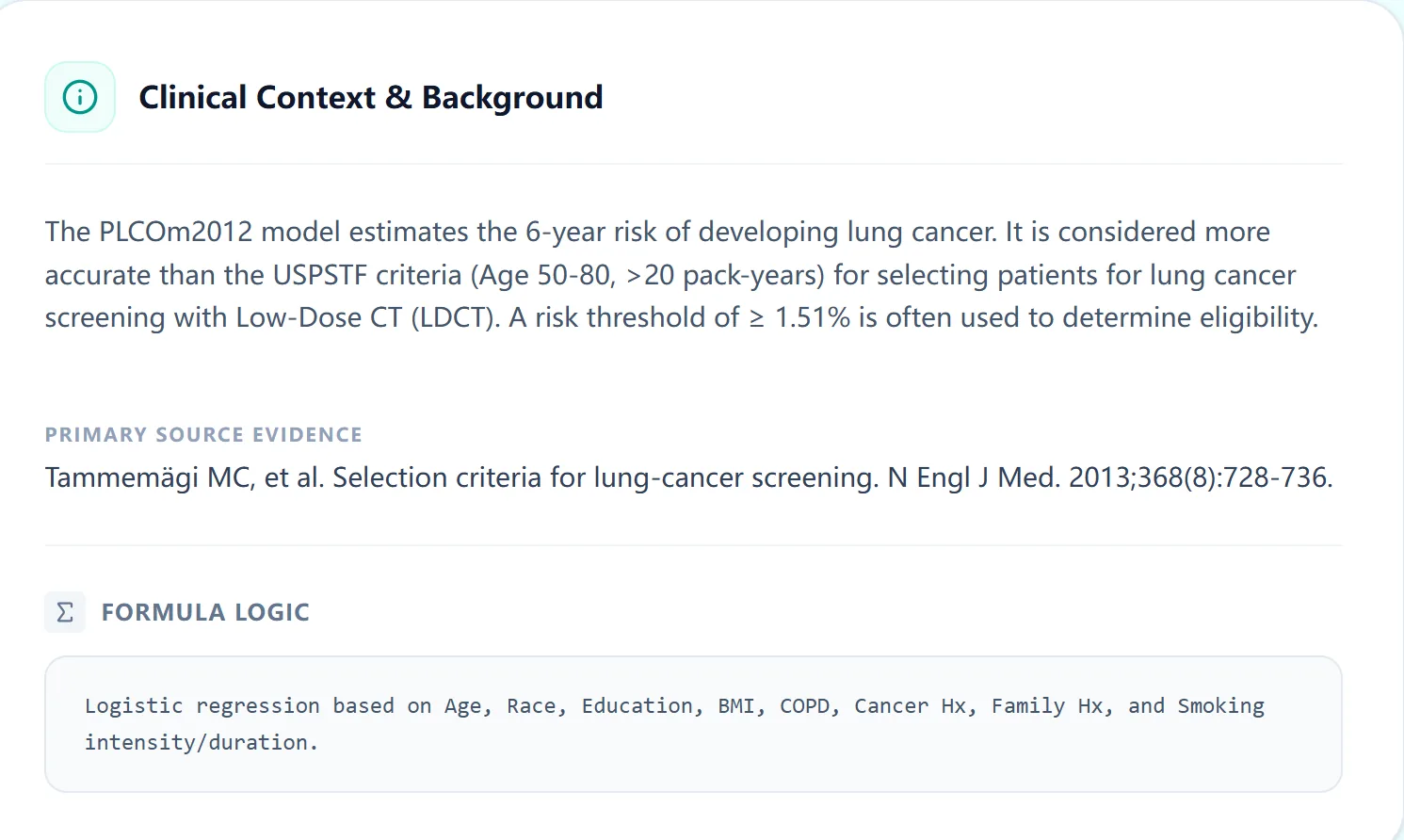
Figure 1. The PLCOm2012 model foundation includes logistic regression weighting of variables derived from the PLCO trial cohort.
3. Clinical Significance: Moving Beyond Standard Criteria
The evolution of lung cancer screening guidelines reflects a shift toward precision medicine. The 2013 USPSTF criteria (ages 55–80, ≥30 pack-years, quit less than 15 years) were groundbreaking but limited. The 2021 USPSTF update expanded eligibility to adults aged 50–80 years with at least 20 pack-years who currently smoke or quit within 15 years, yet categorical criteria can still miss some high-risk patients.3
PLCOm2012 addresses this gap by adding individualized risk estimation to the screening conversation. A 6-year PLCOm2012 risk threshold around 1.51% is commonly cited in model-based screening literature and implementation studies; local programs should still align decisions with current guidelines, patient fitness, and shared decision-making.1, 4
3.1 Reducing Disparities in Screening Eligibility
A critical advantage of PLCOm2012 over categorical criteria is its potential to reduce racial, ethnic, and sex-based disparities. Risk-model approaches may reduce some disparities created by fixed age and pack-year rules because they account for more than smoking intensity alone. Studies comparing PLCOm2012 with categorical criteria have found improved sensitivity in selected racial and ethnic groups, including African American screening cohorts.6
3.2 Optimizing Clinical Workflow and Cognitive Load
On our platform, this entire assessment takes under 30 seconds. You enter the variables, click "Calculate Score," and instantly see the patient's risk percentage and screening eligibility status. This efficiency matters not just for the individual patient, but for MDT workflows, teaching rounds, and quality improvement audits.
4. Evidence and Validation of the PLCOm2012 Model
4.1 The Mathematical Foundation
PLCOm2012 employs logistic regression, a statistical technique that models the probability of a binary outcome based on multiple input variables. Each variable is assigned a weight that reflects its independent association with risk. The final output is an absolute probability.
4.2 Comparing PLCOm2012 to Bach and Spitz Models
| Model | Variables | Strength | Limitation |
|---|---|---|---|
| PLCOm2012 | 9 factors | Prospective validation; NCCN standard | More variables to input |
| Bach | 6 factors | Early validation; simplicity | No family history/COPD; needs asbestos |
| Spitz | Varies | High Specificity (PPV 88.2%) | Lower sensitivity; lacks guideline endorsement |
PLCOm2012 has achieved broad use because it is transparent, clinically interpretable, and has been compared prospectively against categorical screening criteria in screening-selection studies.4
5. Clinical Limitations and Implementation Caveats
Clinicians should be aware of:
- Smoking Accuracy:Relies on self-reported data.
- Family History:Does not differentiate degree of relationship or age of onset.
- Populations:Primarily derived from North American cohorts; calibration and implementation thresholds may vary across populations.
- Time Horizon:Predicts 6-year risk only.
6. How to Use the OncoToolkit PLCOm2012 Calculator
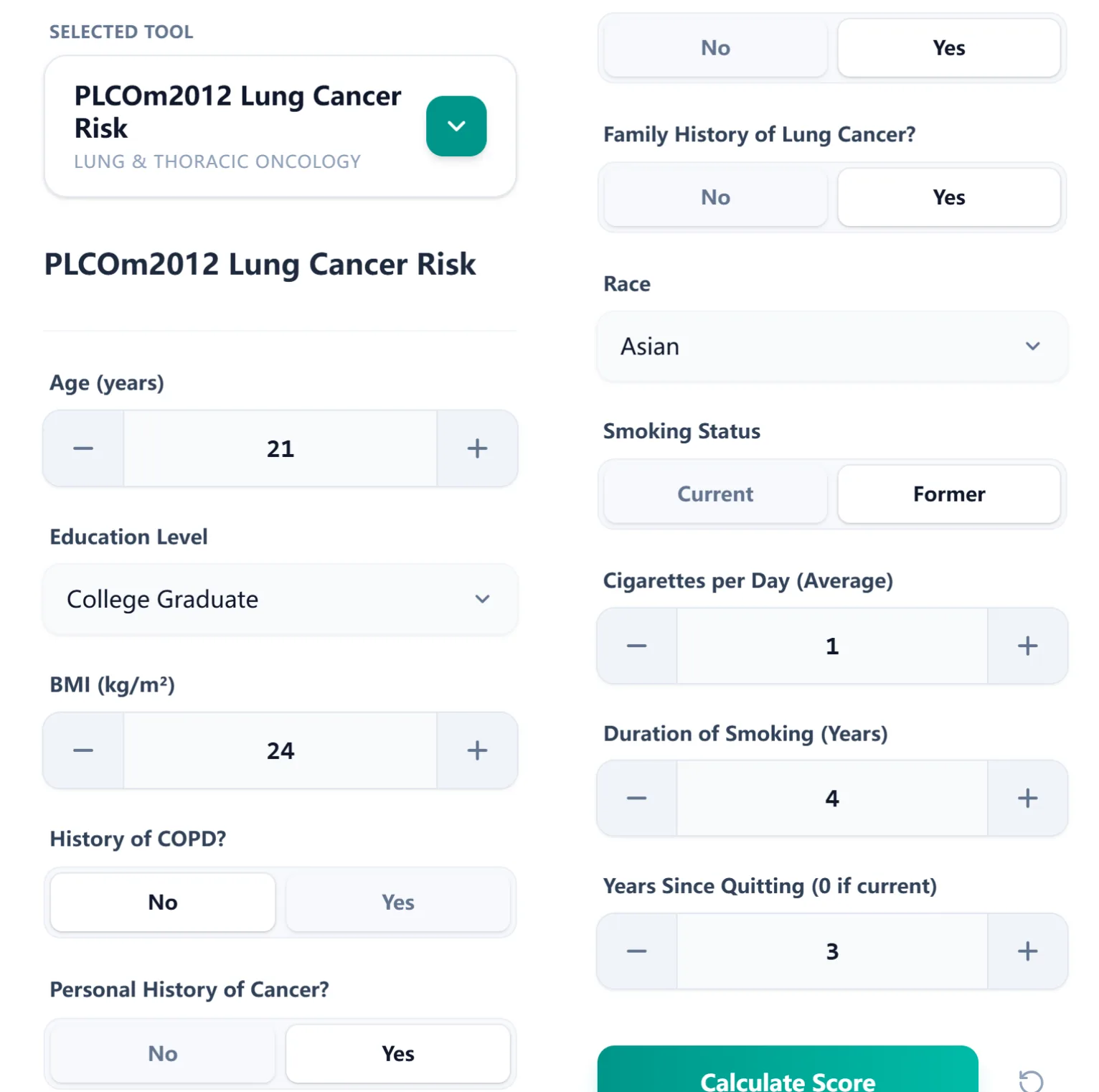
Figure 2. Input interface for PLCOm2012
On OncoToolkit, the process is streamlined:
- Step 1: Data Entry - Enter demographics, medical history, and smoking details.
- Step 2: Calculation - The algorithm generates the individualized 6-year risk in real-time.
- Step 3: Result Interpretation - Receive a color-coded output with NCCN screening eligibility.
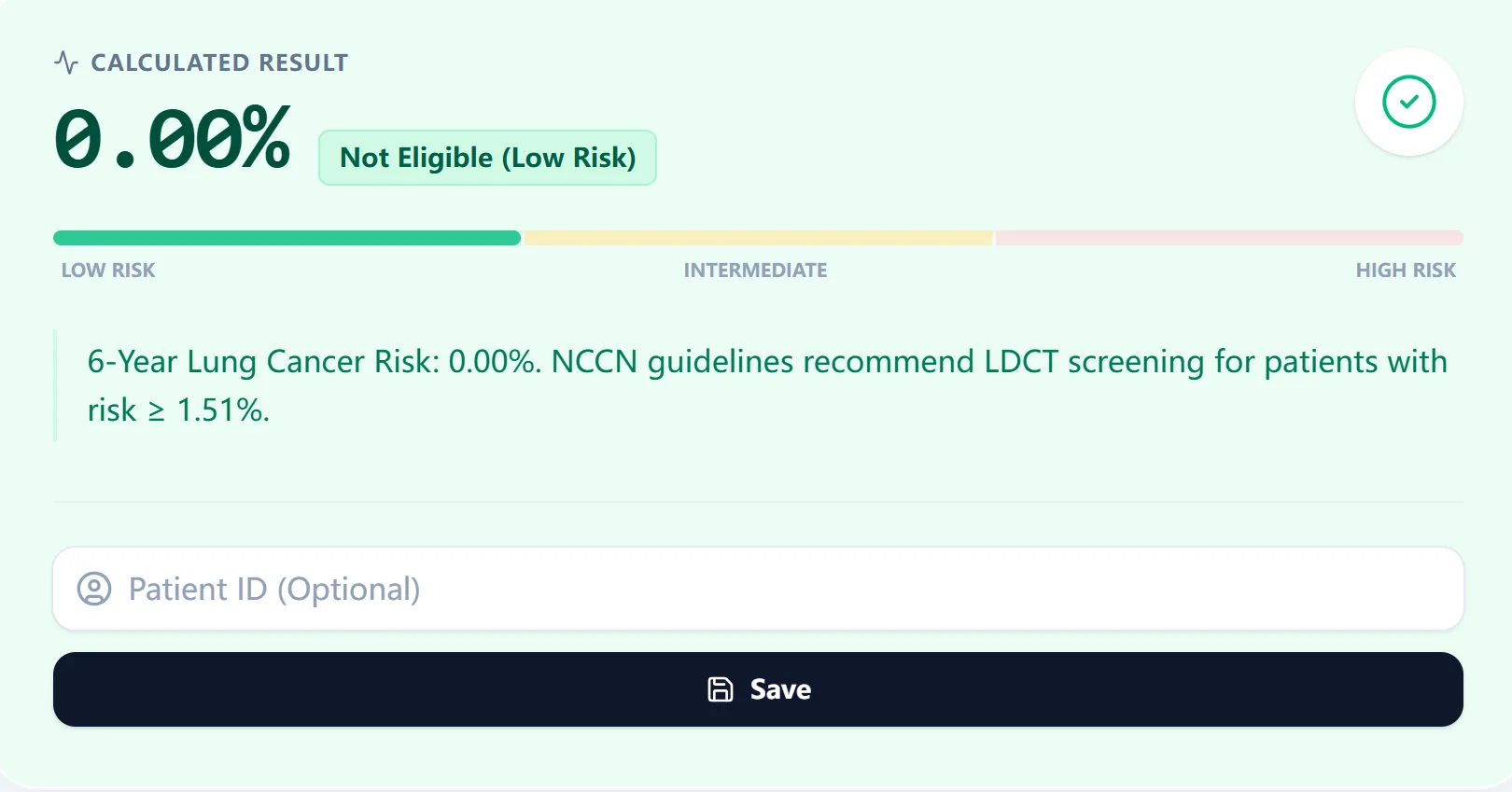
Figure 3. Calculated result example
7. Guideline-Based Risk Stratification Framework
The calculator is grounded in clear, evidence-based thresholds:
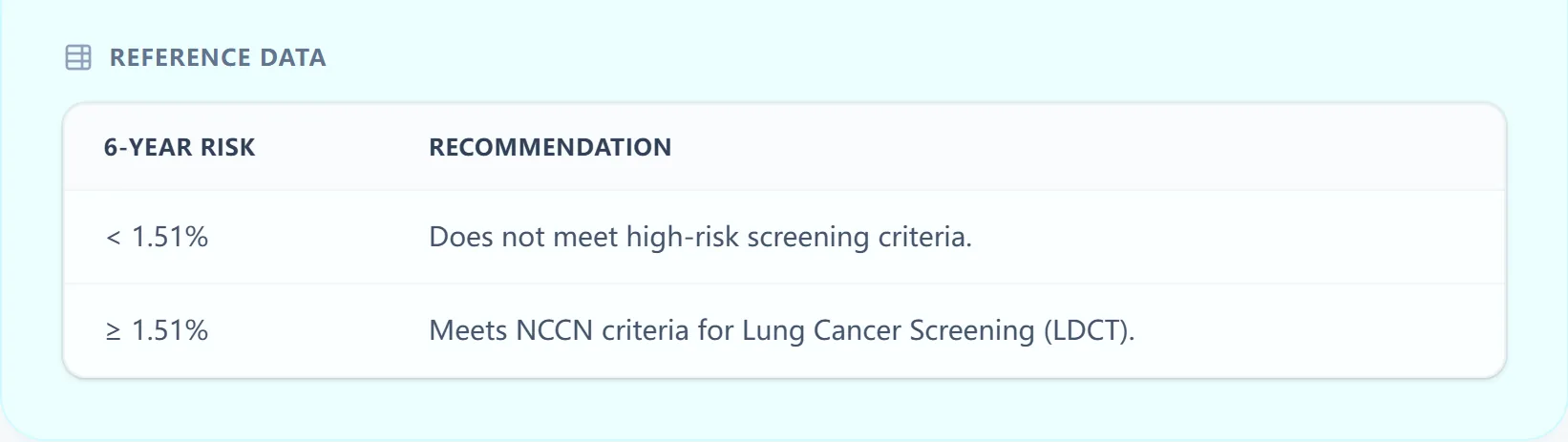
Figure 4. Risk stratification thresholds
8. Supporting Clinical Care, Education, and Research
- Clinical Decision Support: Point-of-care use in outpatient clinics and MDT boards.
- Education: Hands-on practice for residents to understand variable interactions.
- Research: Program evaluation, outcomes research, and quality improvement audits.
9. Frequently Asked Questions (FAQ)
Can PLCOm2012 be used in patients with significant comorbidities?
The model does not incorporate life expectancy. Clinical judgment is essential.
What is the most common mistake when calculating PLCOm2012?
Miscounting pack-years or confusing smoking duration with total pack-years. The model asks for these separately.
Is it validated for non-US populations?
Studies outside the United States support PLCOm2012 performance in several screening settings, but calibration and implementation thresholds can vary by population and program.
10. Conclusion: Integrating Risk-Based Screening
The PLCOm2012 calculator represents a shift toward precise, personalized, transparent lung cancer screening decisions. By embedding this into your practice, you reduce cognitive load and ensure equitable care.
After LDCT
Use Lung-RADS for Screening CT Reports
Translate CT findings into a standardized category and follow-up pathway.
If a Nodule Is Found
Compare Brock, Mayo, and Herder
Use nodule-specific models after imaging identifies a pulmonary nodule.
Ready to Simplify Your Screening Decisions?
Implement the gold-standard PLCOm2012 model in your clinical workflow today.
Try the PLCOm2012 Calculator Now
Free to use. No registration required.
References
- Tammemägi MC, et al. Selection criteria for lung-cancer screening. N Engl J Med. 2013;368:728-736. Source
- Tammemägi MC, et al. Development and validation of a lung cancer risk prediction model. J Natl Cancer Inst. 2011;103:1058-1068. Source
- USPSTF. Screening for lung cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021. Source
- International Lung Screening Trial investigators. Risk model versus USPSTF criteria for lung cancer screening selection. Source
- NCCN Guidelines Insights: Lung Cancer Screening, Version 1.2025. Source
- Risk prediction model versus USPSTF criteria in African American smokers. Source
- OncoToolkit PLCO vs Brock workflow guide. Source